
The term 'overdose' is almost universally used to describe a substance-related death or adverse event. The term is however, dangerously incorrect in the majority of cases.
 Following is an account of what is commonly but incorrectly
referred to as 'overdose'. Approximate reading time: twenty minutes.
Following is an account of what is commonly but incorrectly
referred to as 'overdose'. Approximate reading time: twenty minutes.
THE TRUTH ABOUT 'OVERDOSE' AND THE DANGER OF MIXING DRUGS
INTRODUCTION
The contents of this page is concerned with situations brought about by use of central nervous system depressant drugs and importantly, combinations of these substances. These drugs include alcohol, opioids, GHB, benzodiazepines, barbiturates, and cannabis etc. These are drugs that 'slow' the brain and can induce sedation.
The most dangerous drug in regards to death or injury when taken as the only substance or in combination with others, is alcohol. This is due to its sedating effect, long duration of action (half-life) and the likelihood of vomiting. Entry of stomach contents into the windpipe can impair or prevent breathing.
A very common and under-recognised danger is however, a mixture of different types of 'depressant' drugs. Multiple-drug toxicity (heavy sedation) leading to airway obstruction and asphyxiation, is a common cause of death and injury.
The simple, uninformed and 'spur of the moment' act of taking a second type of 'depressant' drug 'on top' of another, can have devastating consequences. The legal status of any of the substances is of no relevance.
IF YOU INTEND TO TAKE 'DEPRESSANT' DRUGS, THE SAFEST THING TO DO IS TO TAKE A SENSIBLE, MODERATE AMOUNT OF ONE DRUG ONLY.
When more than one drug type is taken, the following situation is possible:
Heavy sedation (being unconscious and unable to be woken) leading to airway obstruction and breathing difficulties. Airway obstruction is a restriction or complete blockage in the throat and/or windpipe that prevents proper breathing. It can be caused simply by the position of your head and jaw and/or vomit. A situation of heavy sedation and airway obstruction is dangerous and can be life threatening.
THIS SITUATION IS NOT RELATED TO TAKING 'TOO MUCH' OF A PARTICULAR SUBSTANCE. IT IS A RESULT OF HAVING A COMBINATION OF DRUGS IN YOUR BLOODSTREAM THAT CAUSES HEAVY SEDATION.
FOR EXAMPLE: You have been drinking alcohol for several hours at a party. You are offered a different class of 'depressant' drug such as some GHB. You sit down after leaving the party, take the substance and become unconscious due to the combination of drugs. Your head falls forward and your airway becomes obstructed.
You are unable to breathe properly and are too sedated to make adjustments to your body position to fix the situation. You then vomit. Breathing becomes impossible because of airway obstruction brought about by the position of your head and the presence of vomit. The chain of events leads to your death.
This was NOT an 'overdose'. It was NOT brought about solely by GHB or alcohol. It was the result of TWO SUBSTANCES taken together causing heavy sedation, which along with the presence of vomit, resulted in airway obstruction and cessation of breathing.
An example of a potentially dangerous multiple-drug toxicity situation involving use of a medication under medical direction and a recreational drug, would be taking an opioid medication for pain relief and then drinking alcohol.
Only when a drug or medication is completely metabolised (broken down), is it safe to take a different class of substance from the perspective of multiple-drug toxicity.
A DANGEROUS TERM
The term 'overdose' has become a universal 'catch-all' word used to describe a substance-related adverse event or death. However, for the majority of incidents, the term is not accurate. Furthermore, use of the term for incidents in which multiple substances were present is not only incorrect, but also dangerously misleading. The term is commonly used in a deliberate way to misrepresent what has actually occurred.
There are two particularly dangerous aspects to the inappropriate use of the term 'overdose':
1. Use of the term incorrectly infers that the biggest danger is taking 'too much' of a particular substance. Usually, the most dangerous circumstance is a combination of substances.
&
2. No mention is made of the most important issue: breathing.
When a person is unconscious due to substance use (and their heart is beating):
THE MOST IMPORTANT ISSUE IS THEIR BREATHING.
It is not 'respiratory depression' that usually presents the immediate danger, it is
AIRWAY OBSTRUCTION
The following assumes that the person is capable of breathing unassisted. The usual scenario for those who are sedated from drug use is that they can breathe unassisted, but as with any unconscious person, are at risk of airway obstruction.
AIRWAY OBSTRUCTION
Airway obstruction is when there is a physical barrier to air entering and exiting the lungs. This means the person cannot breathe properly. The barrier can simply be caused by their head and/or jaw (and therefore tongue) being in the wrong position, the presence of vomit, or a combination of these factors. The result is restricted breathing or breathing stopping completely.
A person cannot actually 'swallow their tongue': it can simply restrict or block a person's airway when they are heavily sedated (unconscious) from substance use and unable to control its position. This usually happens in combination with their head and/or jaw also being in a dangerous position.
Snoring and wheezing sounds are indicative of partial airway obstruction. Gurgling sounds can indicate that stomach contents have entered the throat. This is an emergency situation.
 When a person is conscious (and when they are sleeping) they ensure
satisfactory breathing by subconsciously making adjustments to their head and jaw position (maintaining their airway). However, when a person
is sedated from drug use so as they are unconscious, they can lose the ability to make these adjustments to body position and can subsequently
suffer breathing problems.
When a person is conscious (and when they are sleeping) they ensure
satisfactory breathing by subconsciously making adjustments to their head and jaw position (maintaining their airway). However, when a person
is sedated from drug use so as they are unconscious, they can lose the ability to make these adjustments to body position and can subsequently
suffer breathing problems.
Positioning of structures in the throat such as the tongue, epiglottis and soft palate can prevent adequate breathing. This can be as simple as the position of a person's head. A person can die due to airway obstruction.
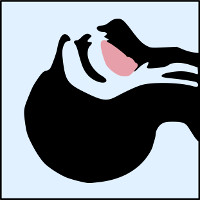
This image shows unobstructed breathing. Air can easily get from the mouth and nose to the lungs and back out again.
In this example, the head is in the 'head tilt' position which is commonly used in first aid when neck injury is not suspected.
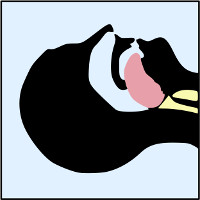
This image shows how structures in the throat including the tongue can block the throat, stopping air getting to and from the lungs.
If this situation is not remedied, the person may suffer brain injury or actually die from lack of oxygen.
(The windpipe is the uppermost passage)
An easy demonstration
If you put your head straight down so your chin is close to your chest and at the same time relax completely, you will experience a degree of airway obstruction. With your head in this position and your jaw relaxed, you will be aware of the unpleasant and disconcerting feeling that you are about to suffocate. The situation could be likened to the kinking of a hose, with your neck and therefore your airway, the 'hose'.
What to do if airway obstruction is present
Regardless of the cause, airway obstruction must be fixed immediately. If someone is unconscious and unable to be roused, medical assistance should be obtained. It is what is done in the period before help arrives that is critical. Basic first aid should be applied with the person positioned correctly and the airway checked for matter that could restrict or prevent breathing.

The best way for unqualified people to manage a breathing, unconscious person who is not suspected of having spinal injuries, is by using the 'recovery position'. This position gives good protection from airway obstruction brought about by structures of the throat and provides a path for liquid to leave the mouth.
What not to do
There are some interventions that provide no assistance at all and are actually dangerous in regards to drug-induced sedation.
 These include: slapping the person's face, putting your fingers in their
mouth in an attempt to retrieve a 'swallowed tongue', putting them in a cold shower and giving other substances in an attempt to 'sober them up'
etc. Body positioning that is dangerous (apart from face down) includes lying flat on their back and sitting (especially with their head falling
forward).
These include: slapping the person's face, putting your fingers in their
mouth in an attempt to retrieve a 'swallowed tongue', putting them in a cold shower and giving other substances in an attempt to 'sober them up'
etc. Body positioning that is dangerous (apart from face down) includes lying flat on their back and sitting (especially with their head falling
forward).
Any person that is unconscious and unable to be roused, for whatever reason, must have their airway monitored and if necessary, supported.
Airway obstruction in the surgical environment
An explanation of airway obstruction in the surgical environment can assist in understanding the situation arising due to substance use. In an operating theatre, people are anaesthetised so as they are unaware of the procedure and pain that it causes. Patients are administered drugs to sedate them to the point that they are unable to be roused (unconscious).
At this point, they are still breathing unassisted but they have lost the ability to maintain their airway i.e. they cannot control the position of their head, jaw and structures such as their tongue. So accordingly, if the position of their head and jaw is not manually maintained by medical personnel, they will almost certainly succumb to asphyxiation (deficient supply of oxygen) due to an obstructed airway.
Obviously, it is impractical for a patient's airway to be manually maintained for the duration of an operation. The answer is to install a breathing tube. This means that the passage of air to and from the patient's windpipe (and therefore lungs) is assured. The patient's tongue and other structures do not present a danger regarding restricting or preventing breathing, as the tube allows and protects the passage of air.
So, in terms of a person's airway, exactly the same thing can occur during heavy sedation from drug use as happens in an operating theatre: airway obstruction. The difference is that when a person has breathing difficulties due to drug use, they usually do not have their airway maintained by others. This is the danger.
MIXING DRUGS: A DANGEROUS PRACTICE
A significant number of deaths and adverse events described as 'overdoses' are not in fact, overdoses. They are not the result of a person simply taking 'too much' of a particular substance. They are a combination of two factors:
1. MULTIPLE-DRUG TOXICITY
(heavy sedation due to a combination of drugs)
&
2. ASPHYXIATION DUE TO AIRWAY OBSTRUCTION
MULTIPLE-DRUG TOXICITY DEATHS AND ADVERSE EVENTS ARE NOT 'OVERDOSES': THEY ARE DUE TO A PERSON TAKING TWO OR MORE DIFFERENT TYPES OF CENTRAL NERVOUS SYSTEM DEPRESSANT DRUGS AND BECOMING SO SEDATED (UNCONSCIOUS) THAT THEY ARE UNABLE TO MAINTAIN THEIR AIRWAY.
THE PERSON CAN LOSE THE ABILITY TO BREATHE PROPERLY. IN THE WORST CASE SCENARIO, THEY ARE NOT ABLE TO BREATHE AT ALL.
MULTIPLE-DRUG TOXICITY
When two or more different types of central nervous system depressant drugs are taken, a situation of heavy sedation can rapidly occur. The amount of each individual drug taken on its own would not normally have presented a problem, but in combination, the resulting sedation can be dangerous.
The person can become unconscious and unable to be woken. In essence, they have become anaesthetised. They are breathing, but are unable to respond to situations that can compromise breathing. The immediate danger is that the person may develop airway obstruction, which can progress to asphyxiation (lack of oxygen).
The situation is often incorrectly portrayed as being due to 'respiratory depression', where the breathing reflex is slowed or ceases due to compromise of the central nervous system. In the vast majority of cases of multiple-drug toxicity, the person is breathing adequately but unable to respond to and prevent airway obstruction.
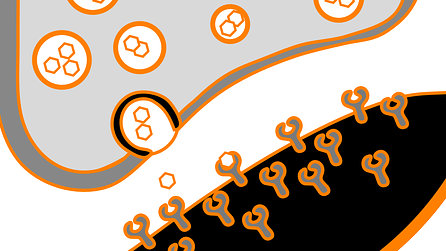
Representation of neuronal junction (synapse)
Regarding the neurological mechanism of multiple-drug toxicity, two common scenarios have the ability to result in dangerous sedation:
 A combination of two drugs that act on the same receptor
system (for example, GABA), but may have different mechanisms of action. An example is alcohol and benzodiazepines.
A combination of two drugs that act on the same receptor
system (for example, GABA), but may have different mechanisms of action. An example is alcohol and benzodiazepines.
A combination of two drugs that act on different receptor systems.
An example is alcohol (GABA system) and opioids (opioid system).
Amongst people who have experience combining drugs, the terms 'dropping' or 'going over' are often used. Apart from the obvious reference to collapse, these terms indicate the speed with which the sedation can occur.
As the term 'overdose' is dangerously incorrect and misleading in many situations, there must be a new term for an event involving drug use, sedation and airway obstruction (or the danger of airway obstruction). Such a term might be Drug-induced Dangerous Sedation Event, or the abbreviation:
DDSE
Opioids and multiple - drug toxicity
 Opioids are the drug class commonly alleged to be associated with
adverse outcomes due to 'overdose'. The common misconception is that if a person takes more heroin (morphine) than usual, they can simply stop
breathing due to 'respiratory depression'. It is clear however, that this scenario is not a reality. It has been clinically proven that
substantial overdose of heroin is not dangerous.
Opioids are the drug class commonly alleged to be associated with
adverse outcomes due to 'overdose'. The common misconception is that if a person takes more heroin (morphine) than usual, they can simply stop
breathing due to 'respiratory depression'. It is clear however, that this scenario is not a reality. It has been clinically proven that
substantial overdose of heroin is not dangerous.
The situation that is directly implicated in adverse outcomes in which opioids are involved is a mixture of drugs: most commonly opioids and alcohol. Asphyxiation due to airway obstruction in the context of heavy sedation can be the consequence of a combination of substances.
FATALITIES INVOLVING COMBINATIONS OF SUBSTANCES
Following are two high profile Australian examples of deaths involving combinations of drugs. The drug common to both cases is alcohol. Neither person can be said to have died due to the effects of an 'overdose' nor solely the effects of an illicit substance. Both incidents have the hallmarks of mixed-drug toxicity: heavy sedation caused by a combination of central nervous system depressant drugs.
This sedation can lead to airway obstruction and asphyxiation. Both deaths continue to be incorrectly described as being due to 'overdoses' of their respective illicit drug. The purpose of these examples is to illustrate the danger of mixing drugs and thereby help prevent deaths and injury.
Dianne Brimble
Dianne Brimble died aboard a cruise ship off the coast of Australia in 2002. An internet search using her name provides multiple references to her dying as a result of GHB and/or an 'overdose of GHB'. The following was documented in the report of the inquest into her death: "[t]he cause of death is the effects of gamma hydroxybutyrate." (1:p4) However, Ms Brimble also had a significant blood-alcohol level (0.127g/dl). (1:p4) The pathologist noted that she "...had vomited prior to death." (1:p4)
Her death cannot be described as having been the result of consumption of one drug or an 'overdose' of one drug (in this case GHB), as alcohol was also involved.
Damien Trimingham
Damien Trimingham died in 1997. An internet search using his name provides multiple references to him dying as a result of a 'heroin overdose'. This is not the case. As stated in a book by his father, Damien "...had an argument with his girlfriend, then a heavy drinking session..., withdrew his last $50 from an ATM and caught the 7.30 p.m. train from Katoomba". (2:p5) He subsequently took an opioid.
There is no basis in fact for the suggestion that he succumbed to a 'heroin overdose' or an 'overdose', as alcohol was also involved.
REFERENCES
1. Inquest into the death of dianne brimble (Glebe Ref: 1638 / 02). Magistrate Jaqueline M. Milledge. (2010)
2. Not my family, never my child. What to do if someone you love is a drug user. Tony Trimingham. (2009)
